 Development
of Left Occipitotemporal Systems for Skilled
Reading in Children After a Phonologically-Based Intervention
Development
of Left Occipitotemporal Systems for Skilled
Reading in Children After a Phonologically-Based Intervention
Bennett A. Shaywitz, Sally E. Shaywitz, Benita A. Blachman, Kenneth R. Pugh, Robert K. Fulbright, Pawel Skudlarski, W. Einar Mencl, R. Todd Constable, John M. Holahan, Karen E. Marchione, Jack M. Fletcher, G. Reid Lyon, and John C. Gore
Background: A range of neurobiological investigations shows afailure ofleft hemisphere posterior brain systems to function properly during reading in children and adults with reading disabilities. Such evidence of a disruption in the normal reading pathways provides a neurobiological target for reading interventions. In this study, we hypothesized that the provision of an evidence-based, phonologically mediated reading intervention would improve reading fluency and the development of the fast-paced occipitotemporal systems serving skilled reading.
Methods: Functional magnetic resonance imaging was used to study the effects of a phonologically based reading intervention on brain organization and reading fluency in 77 children aged 6.1-9A years (49 with reading disability and 28 control subjects). Children comprised three experimental groups: experimental intervention (n = 37), community intervention (n = 12), and community control subjects (n = 28).
Results: Immediately after theyear-long intervention, children taught with the experimental intervention had made significant gains in reading fluency and demonstrated increased activation in left hemisphere regions, including the inferior frontal gyrus and the middle temporal gyrus; 1 year after the experimental intervention had ended these children were activating bilateral inferior frontal gyri and left superior temporal and occipitotemporal regions.
Conclusions: These data indicate that the nature of the remedial educational intervention is critical to successful outcomes in children with reading disabilities and that the use of an evidence-based phonologic reading intervention facilitates the development of those fast-paced neural systems that underlie skilled reading.
Key Words: Reading, dyslexia, fluency, functional magnetic resonance imaging, plasticity, intervention
![]()
| R |
eading disability (developmental dyslexia) is one of the most common neurobehavioral problems affecting children and adults. There is now a strong consensus that the central difficulty in reading disability reflects a deficit within the language system, and more particularly, in a lower-level compo-nent, phonology, which has to do with the ability to access the underlying sound structure of words (Shaywitz 1998; Wagner and Torgesen 1987). In young school-age children, a deficit in phonology represents the most reliable and specific correlate of reading disability (Fletcher et al 1994; Morris et al 1998). Such findings form the basis for the most successful and evidence-based interventions designed to improve reading (Report of the
![]() From the Departments of Pediatrics (BAS, SES, KRP, WEM, JMH, KEM), Neu-rology
(BAS), and Diagnostic Radiology (RKF, PS, RTC, JCG), Yale Univer-sity School
of Medicine; Department of Applied Physics (JCG), Yale Uni-versity; and Haskins
Laboratories (KRP, WEM), New Haven, Connecticut; Department of Psychology
(BAB) and School of Education (BAB), Syra-cuse University, Syracuse, New York;
Department of Pediatrics (JMF), University of Texas-Houston Health Science
Center, Houston, Texas; Child Development and Behavior Branch (GRL), National
Institute of Child Health and Human Development, National Institutes of Health,
Bethesda, Maryland; and the Institute of Imaging Science (JCG) and Department
of Radiology and Radiological Sciences (JCG), Vanderbilt University, Nashville,
Tennessee.
From the Departments of Pediatrics (BAS, SES, KRP, WEM, JMH, KEM), Neu-rology
(BAS), and Diagnostic Radiology (RKF, PS, RTC, JCG), Yale Univer-sity School
of Medicine; Department of Applied Physics (JCG), Yale Uni-versity; and Haskins
Laboratories (KRP, WEM), New Haven, Connecticut; Department of Psychology
(BAB) and School of Education (BAB), Syra-cuse University, Syracuse, New York;
Department of Pediatrics (JMF), University of Texas-Houston Health Science
Center, Houston, Texas; Child Development and Behavior Branch (GRL), National
Institute of Child Health and Human Development, National Institutes of Health,
Bethesda, Maryland; and the Institute of Imaging Science (JCG) and Department
of Radiology and Radiological Sciences (JCG), Vanderbilt University, Nashville,
Tennessee.
Address reprint requests to Dr. Bennett A. Shaywitz, Yale University School of Medicine, Department of Pediatrics, P.O. Box 3333, New Haven, CT 06510-8064.
Received September 18,2003; revised December 17,2003; accepted December 19,2003.
National Reading Panel 2000). According to recent findings (Torgesen et al 1999), provision of an evidence-based intervention at an early stage of reading instruction leads to the development of fluent reading ("the ability to read a text quickly, accurately and with proper expression" (Report of the National Reading Panel 2000), the hallmark of skilled reading.
A range of neurobiological investigations, using postmortem brain specimens (Galaburda et al 1985), brain morphometry (Filipek 1996), diffusion tensor magnetic resonance imaging (MRI) (Klingberg et al 2000), and functional brain imaging in reading-disabled readers (Brunswick et al 1999; Helenius et al 1999; Horwitz et al 1998; Paulesu et al 2001; Rumsey et al 1992, 1997; Salmelin et al 1996; Shaywitz et al 1998) shows a failure of left hemisphere posterior brain systems to function properly during reading. This neurobiological evidence of dysfunction in left hemisphere posterior reading circuits is already present in reading-disabled children and cannot be ascribed simply to a lifetime of poor reading (Seki et al 2001; Shaywitz et al 2002; Simos et al 2000; Temple et al 2000).
Such evidence of a disruption in the normal reading pathways pro vides a neurobiological target for reading interventions. In this study, we hypothesized that the provision of an evidence-based, phonologically mediated reading intervention would improve reading fluency and the development of the fast-paced occipitotemporal systems serving skilled reading. We chose a letter identification task, because we wanted a task that was easy enough for very young disabled readers to perform with high accuracy—we did not want the issue of effort to be a factor in interpreting the results. A number of investigations (reviewed in Scarborough 1998) indicate that in young children, letter identification is the strongest predictor of reading ability. The experimental intervention was adapted from a model used previously in a prevention study with first-grade children (Blachman et al
Methods and Materials
Subjects
Seventy-seven right-handed children, aged 6.1-9.4 years, were recruited for three experimental groups: experimental intervention (EI, n = 37), community intervention (CI, n = 12), and community control subjects (CC, n = 28). Children in the EI group were recruited from area schools in and around Syracuse, New York. Children in the CI and CC groups were recruited in the New Haven, Connecticut metropolitan region from a number of sources, includ-ing referrals from pediatricians, nurses, psychologists, educators, and family physicians, as well as through notices in parent-teacher association bulletins, public libraries, scouting groups, children's toy stores, and community organizations.
Criteria for reading disability were met if a child had a standard score below 90 (below the 25th percentile) on either the Word Identification or the Word Attack subtest of the Woodcock reading achievement tests (Woodcock 1987; Woodcock and Johnson 1989) and on the average of both subtests. The Word subtest assesses an individual’s ability to read real words. The Word Attack subtest consists of nonsense words (pseudowords), and the subject is asked to pronounce the nonwords, which requires use of decoding and phonetic skills. A verbal intelligence quotient (IQ) of 80 or greater as measured on the Wechsler Intelligence Scale for Children-Revised (Wechsler 1981) was required to participate in the study. To ensure good readers and no overlap between groups, a criterion for the CC group was reading above the 39th percentile. The primary outcome variable was reading fluency, as measured by the passage score on the Gray Oral Reading Test (GORT) (Wiederholt and Bryant 1992). The GORT is an oral reading test measuring rate, accuracy, fluency, and comprehension. The test contains short passages, with each story followed by five multiple-choice comprehension questions. Passages increase in difficulty and complexity as students progress through the test. Exclusion criteria consisted of the following: left-handedness, hearing loss, severe articulation problems, severe emotional disturbance, autism, mental retarda-tion, brain injury, neurologic disorders (e.g., epilepsy), and having English as a second language. All subjects gave informed consent before entry into the study, which was approved by the Human Investigation Committee of the Yale University School of Medicine and, for the EI subjects, by the Institutional Review Board of Syracuse University. Specifically, a detailed explanation of the study was provided to each of the parents individually on two separate occasions, and an opportunity was provided to ask questions and express concerns. The parents then signed the consent forms if they wanted their child to participate in the program. The children, who ranged from 6 to 9 years of age, were then provided with an explanation of the entire process and an opportunity to ask questions by a member of the research staff. They were then asked verbally if they were willing to participate in the program or if they were concerned about any part of the process. A child who stated that he or she did not want to participate would have been excluded; however, all of the children gave verbal permission and were actually eager to participate.
Community Intervention
This group of children met criteria for reading disability and did not receive the intervention protocol. They received a variety of interventions commonly provided within the school setting, includ-ing remedial reading (83%), resource room (50%), special education (33%), modified classroom (33%), speech and language (42%), remedial supportive (17%), and tutoring (83%). Within the CI group, 83% (10 of 12) received more than one school intervention. Intervention frequency ranged from 1 day each week to 4 days each week and lasted between 15 and 50 minutes. Specific, systematic, explicit phonologically based interventions comparable to the experimental intervention were not used in any of school programs that were provided to the community group.
xperimental Intervention
The experimental intervention (Blachman et al 2003) was delivered to children in their home schools in and around Syracuse, New York. Second- and third-grade poor readers were provided with 50 minutes of daily, individual tutoring that was explicit and systematic and focused on helping children under-stand the alphabetic principle (how letters and combinations of letters represent the small segments of speech known as pho-nemes). Knowledge of the alphabetic principle has been shown to lead to more accurate and fluent word recognition, skills that are critical to reading comprehension (Snow et al 1998). Conse-quently, our intervention provided daily opportunities to integrate word-level skill instruction with text-based reading to support fluency and comprehension. Each lesson was built around a five-step plan that included 1) a review of sound-symbol associations (e.g., giving the name, sound, and key word for each letter, as in "a says /a/ as in apple"); 2) practice in phoneme analysis and blending by manipulating letter cards or scrabble tiles to make new words (e.g., changing sat to sap to sip to slip); 3) timed reading of previously learned words to develop fluency; 4) oral reading of stories; and 5) dictation of words with phonetically regular spelling-sound patterns (e.g., chap, spin). In this last step, children were encouraged to stretch out the word (say it slowly) before spelling it, to emphasize the phonologic and orthographic connections. In the final few minutes of the lesson, tutors could add extended activities, such as additional text reading, writing, or games to reinforce skills. Children developed accuracy and fluency by learning the six basic syllable patterns in English (e.g., closed syllables, as in hat and flag; final "e" syllables, as in lake and slide; open syllables, as in he and the si in silent; vowel team syllables, as in train and spoil; vowel + r syllables as in car and perch; consonant + le syllables, as in tumble and needle). As children became more proficient, they progressed from reading single-syllable words to reading multi-syllable words made up of the previously learned syllable types (e.g., perplex, Valentine). Children practiced reading both de-codable books (books that include a high percentage of words with phonetically regular spelling-sound patterns) and trade books that do not emphasize phonetically regular text (e.g., traditional stories that appeal to children of this age, such as the Arthur series by Marc Brown). As reading proficiency increased, the amount of time spent reading phonetically controlled text decreased, and a wider variety of both narrative and expository texts were introduced to increase fluency, comprehension, and a sense of enjoyment.
Children received 8 months of intervention between the pretests administered in late September and the posttests in late May. They continued to receive regular classroom reading instruction, but during the experimental treatment year they did not receive any other remedial reading assistance at school. That
is, the experimental intervention described above replaced any out-of-classroom remedial reading that the school might have otherwise provided by either a reading specialist or special-education teacher. Children participated, on average, in 105 hours of tutoring (range 86-115 hours). Tutoring was provided by 12 certified teachers, who participated in an extensive training program at Syracuse University. To monitor treatment fidelity, each child was observed an average of nine times during the year, and tutors audiotaped one lesson per week per child. Two independent raters listened to two tapes per child (one from a 3-week period in the fall and one from a 3-week period in the spring) and indicated that 90% of the lessons included all required steps. There was 100% interrater agreement.
Procedure
Children in all groups were imaged before and immediately after intervention. We planned to image all participants a third time, 1 year after the intervention was complete. We were able to image 25 of the children in the EI group for this third functional (f)MRI. Only two children in the CC group and two children in the CI group returned for the third fMRI; data are shown for the EI group for this third year.
Functional ImagingTasks
We used fMRI to examine brain activation patterns while the subjects engaged in a cross-modal letter-identification task. This task was different from the Woodcock-Johnson letter-word iden-tification task, in which subjects simply identify a letter or a word. In contrast, the imaging task involved forced-choice letter iden-tification. Specifically, on each trial, the child heard an auditory spoken letter name (e.g., "B") followed 1000 msec later by two visual target letters (e.g., [ B T ]) and pressed one of two response keys to identify the matching letter. Two kinds of visual stimuli were used: 1) phonologically dissimilar target (e.g., [ B K ]); and 2) highly confusable target (e.g., [ B T ]); because responses were similar for phonologically similar and dissimilar target trials, primary analyses collapse across this factor. A baseline task was also used to control for sensory and motor responses. On these trials, the child heard a 220-Hz tone, followed 1000 msec later by two visual target symbols, a period and an asterisk, arranged as either [ . * ] or [ * . ]. The child pressed a response key to identify the position of the asterisk. Visual stimuli were presented for 1000 msec; trial length was 3670 msec. Trials were presented in a block design, with two activation blocks (letter trials) of 10 trials each surrounded by three baseline blocks (asterisk trials) of five trials each. Subjects lay supine in the imaging system, looking up through a prism at a screen that was attached to a gantry. Stimuli were back-projected onto the screen with a liquid crystal display (LCD) projector connected to a Macintosh PowerPC computer (Apple Computer, Cupertino, California) with Psyscope (Cohen et al 1993). Accuracy scores (percent correct) and reaction time were obtained on the letter and asterisk trials and analyzed in two three-factor analyses of variance (ANOVAs) (year [preintervention vs. immediately postintervention] X task [letter vs. asterisk] X group [CC, CI, EI]), with repeated measures on the first two factors. Simple main effects were tested with ttests. Neither accuracy nor reaction time differed between groups.
Functional Imaging Parameters
Functional imaging was performed on a 1.5-Tesla SignaLX MRI system from General Electric Medical Systems (Waukesha, Wiscon-sin). Before functional imaging, 10 axial-oblique T1-weighted ana-tomic images were prescribed parallel to the intercommissural line on the basis of sagittal T1-weighted localizer images. Axial-oblique
images were obtained at the same relative slice location in each subject, extending from the inferior aspect of the temporal lobes to the parietal convexity. Activation images were collected with single shot, gradient echo, echo planar acquisitions (flip angle, 60°; echo time, 60 msec; repetition time, 2000 msec; field of view, 40 X 20 cm; 8-mm slice thickness, 0-mm gap; matrix size, 128 X 64; single excitation) in the same slice locations used for anatomic images. In each of the imaging runs, 66 images per slice location were collected after starting with four preparatory radiofrequency pulses to equilibrate the magnetization.
Functional Imaging Data Analysis
Data analysis was performed with software written in MAT-LAB (MathWorks, Natick, Massachusetts). Before statistical analysis, the images from each run were motion corrected for three translation directions and for the three possible rotations (Friston et al 1996). Six images at each slice location in a run were discarded to account for variation in signal intensity that occurred from the hemodynamic changes in response to a task transition. The remaining images (60 images per slice location per run) were spatially filtered with a Gaussian filter with a full-width half-maximum value of 6.25 mm. With t statistics corrected for linear drift (Skudlarski et al 1999), a t value for each voxel in individual subjects was obtained by comparing images from the activation task with the images from the baseline task. These t test comparisons were used to create activation maps that compared activation and baseline for each subject. Both the activation maps and the anatomic images from individual subjects were transformed by in-plane transformation and slice interpolation into a normalized three-dimensional grid defined by Talairach and Tournoux (1988).
Results
Behavioral Results
Demographic characteristics, IQ data for preintervention, and reading scores for preintervention, immediate postintervention, and 1 year postintervention are shown in Table 1. The primary outcome variable was reading fluency as measured by the GORT (Wiederholt and Bryant 1992) passage score, a combination of accuracy and rate. Groups were similar in age [F(2,74) = .59, p > .55] but differed in mother's education, a frequently used measure of socioeconomic status [F(2,74) = 4.58, p < .013]. Pairwise comparisons revealed that the mother's education level in the CC group was significantly higher than in the EI group (Bonferroni-corrected p = .012). Analyses of preintervention data indicated that, not surprisingly, the CC group demonstrated significantly higher scores than either reading-disabled group (EI or CI) in verbal IQ (Wechsler 1974) [F(2,74) = 49.45, p < .001] and in word (Word ID) and pseudoword (Word Attack) reading (Woodcock and Johnson 1989) [Word ID: F(2,74) = 134.06, p < .001; Word Attack: F(2,74) = 144.83, p < .001]. Similar differ-ences at preintervention were noted on the GORT measures: accuracy [F(2,70) = 78.80, p < .001]; rate [F(2,70) = 117.22, p < .001]; comprehension [F(2,700 = 43.10, p < .001]; and passage [F (2,70) = 108.71, p < .001]. There were no significant differences between EI and the CI groups for any IQ or reading scores at preintervention. Analyses of postintervention data indicated that an ANOVA of the gain in GORT passage scores for the three groups was statistically significant [F(2,69) = 6.34, p = .003]. Pairwise comparisons revealed that the gain by the EI group was significantly greater than that of the CI group (Bonferroni-corrected p = .005). The two other comparisons (CC/EI; CC/CI) were not statistically significant. In-magnet accuracy (percent
correct) and reaction time was obtained on the letter-matching task used in the imaging. Neither accuracy nor reaction time differed between groups. Blachman et al (2003) discuss the behavioral outcomes on a broader range of issues.
fMRI Results
The activation maps from individual subjects were used as a derived measure of task-related activity. The maps were combined by averaging the mean t values of a voxel across subjects within each of the three groups. In this way, composite activation maps were obtained that compared activation—baseline for each group, preintervention, and immediately postintervention. The second
stage of the analysis involved comparing postintervention to preintervention. To avoid the need to assume a specific distribution and variance of the data, a randomization procedure was used to
estimate p values of the group composite maps (Manly 1997). To
randomize, the sign of the activation measure for each voxel, which is the mean t value, was reversed in randomly generated subsets of subjects. The activation measure was then recalcu-lated. This procedure was repeated 1000 times, generating a distribution of the activation measure. The proportion of times
that the observed activation measure was more extreme than a randomized value represents a p value. It is the proportion of times we would expect to obtain a mean activation as large as or larger than the one obtained if the null hypothesis (no difference between tasks) were true. The p value at each voxel (p < .05) was then overlaid on the mean anatomic image for display.
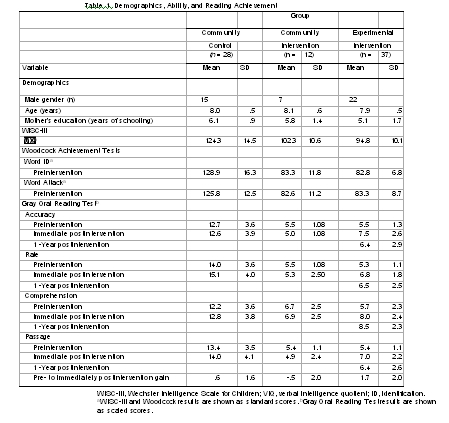
Differences between the immediate postintervention and the preintervention fMRI data are shown in Figure 1. Results are shown as the statistical comparison between groups for the change between preintervention and immediately postintervention. Compared with CI, both CC (Figure 1, middle column), and EI (Figure 1, right column) subjects demonstrated increased activation in left hemisphere regions, including the inferior frontal gyrus and the posterior aspect of the middle temporal gyrus. The results for the CC and EI groups are very similar (Figure 1, left column) except for an increase in activation in the caudate nucleus. This finding suggests that both the CC and EI groups developed reading systems from pre- to immediately postintervention to the same degree, except for the findings in the caudate. At this time we do not have an explanation for this finding. One year after the experimental intervention had ended
| |
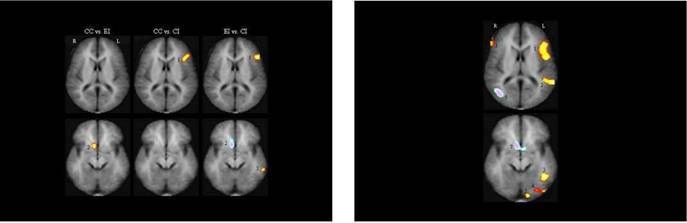
Figure 1. Composite contrast maps demonstrating the interaction of study group and intervention on brain activation patterns. Red-yellow indicates the differences in brain activation between year 1 and year 2 that were more active (p = .05) in the first group compared with the second; blue-purple indicates the differences in brain activation between year 1 and year 2 that were more active (p = .05) in the second group compared with the first. For example, the left column (community control group [CC] vs. experimental intervention group [EI]) indicates how the brain activation differences in year 1 and 2 in the CC group compared with the brain activation differences in year 1 and year 2 in the EI group. The slice locations are 12 and -4 in Talairach space.The legend for brain activation (Talairach x,y,z,coordinates in parentheses) is as follows: 1, inferior frontal gyrus (41,23,12); 2, caudate nucleus (-7,10, -4); and 3, posterior aspect of the middle temporal gyrus (58, -38, -4). CI, community intervention group.
Figure 2. Composite maps indicating the difference in activation between year 3 and year 1 in the EI study group (n = 25). Red-yellow indicates brain regions that were more active (p = .05) in the third year; blue-purple indi-cates brain regions that were more active (p = .05) in the first year. The slice locations are 12 and -4 in Talairach space. Brain regions (Talairach x, y, z, coordinates in parentheses) more active in the third year compared with the first were as follows: 1, bilateral inferior frontal gyri (±41,23,12); 2, the left superior temporal sulcus (51, -42, 12); 3, the occipital temporal region involving the posterior aspects of the middle and inferior temporal gyri and the anterior aspect of the middle occipital gyrus (42, -49, -4); 4, the inferior occipital gyrus (34, -71, -4); and 5, the lingual gyrus (13, -88, -4). The brain regions more active in the first year compared with the third year were 6, the right middle temporal gyrus (-35, -69, 12); and 7, the caudate nucleus (-7,10, -4).
(Figure 2), compared with their preintervention images, EI subjects were activating bilateral inferior frontal gyri, left superior temporal sulcus, the occipital temporal region involving the posterior aspects of the middle and inferior temporal gyri and the anterior aspect of the middle occipital gyrus, the inferior occipital gyrus, and the lingual gyrus.
The thresholded voxel-based activation maps in Figures 1 and 2 are presented for the purpose of display of the spatial distribution of these differences. The voxelwise threshold (p < .05) on these maps takes into account all of the processing steps involved in terms of smoothing, registration, interpolation, and cluster filtering. Applying these processing steps to simulated white noise distributions produced no activations through 10,000 iterations. This suggests that the results shown are unaffected by the multiple comparison problem. To validate the significance of the effect, we defined regions of interest anatomically, focusing on regions (Talairach coordinates for centers of mass) in the inferior frontal gyrus (49, 11, 12), parietotemporal region (51, — 28, 12), and occipitotemporal region (52, —45, —4), which previous studies indicate are critical for reading (Shaywitz et al 2002). Within these regions, the sum of the percent signal change in the activated voxels was used as a measure of activation. For each of the three anatomically defined regions, the activation was found to be significantly (p < .01) greater in year 2 compared with year 1, and significantly greater (p < .001) between year 3 and year 1. For these three regions of interest, group differences between year 2 and year 1 were significant in the inferior frontal gyrus region for CC versus CI (p = .007) and EI versus CI (p = .04), and in the occipitotemporal region for EI versus CI (p = .02). This corroborates the significant differences observed between the groups in the voxel-based maps shown in the figures.
Discussion
These findings indicate that the nature of the remedial edu-cational intervention is critical to successful outcomes in children with reading disabilities and that the use of an evidence-based phonologic reading intervention facilitates the development of those fast-paced neural systems that underlie skilled reading. In this study, a phonologically based reading intervention leads to the development of neural systems both in anterior (inferior frontal gyrus) and posterior (middle temporal gyrus) reading systems. Converging evidence from a number of lines of inves-tigation indicates that a portion of the posterior reading systems, the occipitotemporal area, is critical for the development of skilled reading and functions as an automatic, instant word recognition system, the visual word form area (Cohen et al 2000, 2002; Dehaene et al 2002). In this region, brain activation increases as reading skill increases (Shaywitz et al 2002); this region responds preferentially to rapidly presented stimuli (Price et al 1996), responds within 150 msec after presentation of a stimulus (Salmelin et al 1996), and is engaged even when the word has not been consciously perceived (Dehaene et al 2001). It is this occipitotemporal region that continued to develop 1 year after the intervention had ended (Figure 2). In addition to the changes in posterior brain regions, both the CC and EI groups showed changes in anterior activation. Such findings are conso-nant with reports that anterior brain systems, especially involving regions around the inferior frontal gyrus, have been implicated in reading both in individuals with brain lesions (Benson 1977) as well as in functional brain imaging studies (Brunswick et al 1999; Corina et al 2001; Georgiewa et al 1999; Gross-Glenn et al 1991; Paulesu et al 1996; Rumsey et al 1997; Shaywitz et al 1998). In addition, as shown in Figure 2, in the EI group, two regions were
more active preintervention than 1 year after the experimental intervention had ended: the right middle temporal gyrus and the caudate nucleus on the right. Such findings suggest that these two right-sided systems might be used initially to compensate for the disruption in left-sided posterior systems. With application of an evidence-based reading intervention and development of left hemisphere systems for reading, the right-sided compensatory systems were no longer necessary.
This is the first imaging study of a reading intervention in either children or adults that reports its effects on reading fluency, a critical but often neglected reading skill (Report of the National Reading Panel 2000). It is also the largest imaging study of a reading intervention and the first report of the effects of a reading intervention on fMRI in children that examined not only reading-disabled children who received an experimental reading intervention but also reading-disabled children who did not receive such an intervention. Previous studies on the effects of a reading intervention on neural systems in reading disability were informative but limited to smaller studies in adults, magnetoen-cephalography and magnetic resonance spectroscopy in children, and an fMRI study in only reading-disabled children without a nonexperimental comparison group. Two studies from the same investigative group have used fMRI to examine the effects of a commercial reading program (Fast Forword), first on adults and then in children with dyslexia. The first study examined three adults with dyslexia who received Fast Forword training during a task requiring that subjects respond to a high-pitched stimulus. After 33 training days, two of the three subjects demonstrated greater activation in the left prefrontal cortex after training compared with before training, and these two adults also showed improvement on both rapid auditory processing and audi-tory language comprehension after training; the one adult who did not show a change in fMRI after training failed to show behavioral changes (Temple et al 2000). In a more recent study, immediate short-term improvement in reading accuracy and brain activation changes were observed in 20 children with dyslexia, changes that included the areas observed in our study, as well as in right hemisphere and cingulate cortex (Temple et al 2003). Richards et al (2000) used proton MR spectroscopy to measure brain lactate concentrations at two time points, 1 year apart, in eight dyslexic and seven control boys before and after 3 weeks of a phonolog-ically based reading intervention. Before treatment, dyslexic boys demonstrated increased lactate concentration (compared with control subjects) in the left anterior quadrant during a phonologic task. After treatment, brain lactate concentrations were no different in the dyslexic and control boys, and reading improved after treatment. More recently, this same group re-ported fMRI changes in areas similar to those reported here, after 28 hours of an intensive phonologic and morphologic reading intervention (Aylward et al 2003).
Simos et al (2002) used magnetoencephalography in eight children with dyslexia and eight control subjects before and after 8 weeks of a phonologically based reading intervention. Before intervention, the dyslexic readers demonstrated little or no activation of the posterior portion of the superior temporal gyrus. After intervention reading improved and activation increased in the left superior temporal gyrus.
Findings here with a reading intervention suggest plasticity of the neural systems for reading in children and parallel those observed after a variety of therapies in individuals with stroke (Carey et al 2002) and after surgical removal of a hemisphere in a child with Rasmussen's syndrome (Hertz-Pannier et al 2002). It is reason-able to suppose that these differences in plasticity reflect Gilbert's
view (Gilbert et al 2001) that the "ability of a given brain structure to participate in alteration of topography depends on a preexist-ing framework of connections," and this framework changes with maturation. For example, as children mature, brain activation for "local" in contrast to "global" processing becomes more lateralized (Moses et al 2002). Importantly, the effects of the experimental intervention on the activation of the occipitotem-poral word form area shown to be critical for skilled reading in children (Shaywitz et al 2002) are similar to the co-occurrence of visuospatial proficiency and cortical specialization reported in adults. Thus, Gauthier and associates (Gauthier 2000; Gauthier et al 2000) have demonstrated a progressive increase of activation of the right hemisphere fusiform face area and right lateral occipital cortex with increasing proficiency in identifying novel face-like stimuli they called "Greebles." The current findings suggest that, as with recognition of Greebles, an intervention that improved proficiency in reading was the most important element in functional organization of the neural systems for reading. Such findings have important implications for understanding the effect on neural systems of phonologically based reading programs for young children that have been shown to be effective in the educational equivalent of clinical trials (Report of the National Reading Panel 2000).
A strength of the current report is that in addition to a community control group we also compared the experimental intervention to a community intervention in an effort to minimize the confounding effects of improvement in performance over time or as a result of practice. Another strength relates to the 1-year postintervention follow-up, a time considered critical by Torgesen et al (2001) in studies of the effects of reading interventions on reading outcome. To examine this effect, children in the EI group were studied 1 year after the intervention had ended to determine whether the effects observed immedi-ately after the intervention had ended were lasting. The design intended to study children in the CC and CI group on a third occasion also. A limitation of this report is that in contrast to the parents of the children in the EI group, who were enthusiastic about their children's progress in reading, parents of children in the CC and CI groups were reluctant to return with their children for a third fMRI. Thus, for this third time period, we were not able to compare children in the EI group to those in the CI or CC groups. We suggest that future studies of this kind compare two experimental reading interventions rather than the experimental and community intervention used here. We believe that the smaller number of children in the CI group compared with the EI group reflect a problem inherent in such studies: parents of struggling readers are reluctant to have their children participate in a study unless their children are offered the possibility of receiving effective reading interventions. We think that when parents and children feel that they are receiving an effective treatment, they will be more motivated to enroll in and continue to participate in such a study.
In summary, these data demonstrate that an intensive evidence-based (phonologic) reading intervention brings about significant and durable changes in brain organization, so that brain activation patterns resemble those of typical readers, with the appearance of the left occipitotemporal area and improvement in reading fluency. These data have important implications for public policy regarding teaching children to read: the provision of an evidence-based reading intervention at an early age improves reading fluency and facilitates the development of those neural systems that underlie skilled reading.
www.elsev932 BIOL PSYCHIATRY 2004;55:926-933
This work was supported by grants from the National Institute of Child Health and Human Development (PO1 HD 21888 and P50 HD25802) to BAS and SES. The experimental intervention was supported by a subcontract ofGrant P50 HD25802 to BAB. At Yale, we thank Carmel Lepore, Hedy Sarofin, and Terry Hickey for their invaluable help in imaging subjects. We also thank Cheryl Lacadiefor her help with data analysis. AtSyracuse University, we thank Dr. Shiela Clonan, project coordinator for the experimental intervention.
Aylward EH, Richards TL, Berninger VW, Nagy WE, Field KM, Grimme AC, et al (2003): Instructional treatment associated with changes in brain activation in children with dyslexia. Neurology 61:212-219. Benson D (1977): The third alexia. Arch Neurol34:327-331.
Blachman BA, SchatschneiderC, Fletcher JM, Clonan SM (2003): Early reading intervention: A classroom prevention study and a remediation study.In: Foorman BR, editor. Preventing and Remediating Reading Difficulties:Bringing Science to Scale. Timonium, MD: York Press, 253-271.
Blachman BA, Tangel DM, Ball EW, Black R, McGraw CK (1999): Developing phonological awareness and word recognition skills: A two-year intervention with low-income, inner-city children. Reading and Writing: An Interdisciplinary Journal 11:239 -273.
Brunswick N, McCrory E, Price CJ, Frith CD, Frith U (1999): Explicit and implicitprocessing of words and pseudowords by adult developmental dyslexics: A search for Wernicke's Wortschatz. Brain 122:1901 -1917.
Carey JR, Kimberley TJ, Lewis SM, Auerbach EJ, Dorsey L, Rundquist P, Ugurbil K (2002): Analysis of fMRI and fingertracking training in subjects withchronic stroke. Brain 125:773-788.
Cohen JD, MacWhinney B, Flatt M, Provost J (1993): PsyScope: A new graphic interactive environment for designing psychology experiments. Behav Res Methods Instruments Comput 25:257-271.
Cohen L, Dehaene S, Naccache L, Lehericy S, Dehaene-Lambertz G, Henaff MA, Michel F (2000): The visual word form area: Spatial and temporal characterization of an initial stage of reading in normal subjects and posterior split-brain patients. Brain 123:291-307.
Cohen L, Lehe´ricy S, Chochon F, Lemer C, Rivaud S, Dehaene S (2002):Language-specifictuning of visual cortex? Functional properties of the Visual Word Form Area. Brain 125:1054-1069.
Corina DP, Richards TL, Serafini S, Richards AL, Steury K, Abbott RD, et al (2001): FMRI auditory language differences between dyslexic and able reading children. Neuroreport 12:1195-1201.
Dehaene S, Le Clec'H G, Poline J, Le Bihan D, Cohen L (2002): The visual word form area: A prelexical representation of visual words in the fusiform gyrus. Neuroreport 13:1 -5.
Dehaene S, Naccache L, Cohen L, Bihan DL, Mangin JF, Poline JB, Riviere D (2001): Cerebral mechanisms of word masking and unconscious repetition priming. Nat Neurosci 4:752-758.
Filipek P (1996): Structural variations in measures in the developmental disorders. In: Thatcher R, Lyon G, Rumsey J, Krasnegor N, editors. Developmental Neuroimaging: Mapping the Development of Brain and Behavior. San Diego: Academic Press, 169-186.
Fletcher JM, Shaywitz SE, Shankweiler DP, Katz L, Liberman IY, Stuebing KK, et al (1994): Cognitive profiles of reading disability: Comparisons of discrepancy and low achievement definitions. J Educ Psychol 86:6-23.
Friston K, Frith C, Poline JB, Heather J, Frackowiak R (1996): Spatial registration and moralization of images. Hum Brain Mapp 2:165-189.
Galaburda AM, Sherman GF, Rosen GD, Aboitiz F, Geschwind N (1985):Developmental dyslexia: Four consecutive patients with cortical anomalies. Ann Neurol 18:222-233.
Gauthier I (2000): What constrains the organization of the ventral temporal cortex. Trends Cogn Sci 4:1 -2.
Gauthier I, Tarr M, Moylan J, Skudlarski P, Gore JC, Anderson A (2000): The fusiform "face area" is part of a network that processes faces at the individual level. JCogn Neurosci 123:495-504.
Georgiewa P, Rzanny R, Hopf JM, Knab R, Glauche V, Kaiser WA, Blanz B (1999): fMRI during word processing in dyslexic and normal reading children. Neuroreport 10:3459-3465.
Gilbert C, Sigman M, Crist R (2001): The neural basis of perceptual learning.Neuron 31:681-697.
Gross-Glenn K, Duara R, Barker WW, Loewenstein D, Chang JY, Yoshii F, et al (1991): Positron emission tomographic studies during serial word-reading by normal and dyslexic adults.J Clin Exp Neuropsychol 13:531-544.
Helenius P, Tarkiainen A, Cornelissen P, Hansen PC, Salmelin R (1999): Disso-ciation of normal feature analysis and deficient processing of letter-strings in dyslexic adults. Cereb Cortex4:476-483.
Hertz-Pannier L, Chiron C, Jambaque I, Renaux-Kieffer V, Van de Moortele PF, Delalande O, et al (2002): Late plasticity for language in a child's non-dominant hemisphere: A pre- and post- surgery fMRI study. Brain 125:361-372.
Horwitz B, Rumsey JM, Donohue BC (1998): Functional connectivity of the angular gyrus in normal reading and dyslexia. Proc Nat Acad Sci USA 95:8939-8944.
Klingberg T, Hedehus M, Temple E, Salz T, Gabrieli JD, Moseley ME, Poldrack RA (2000): Microstructure of temporo-parietal white matter as a basis for reading ability: Evidence from diffusion tensor magnetic resonance imaging. Neuron 25:493-500.
Manly B (1997): Randomization, Bootstrap and Monte Carlo Methods in Biology. London: Chapman & Hall.
Morris RD, Stuebing KK, Fletcher JM, Shaywitz SE, Lyon GR, Shankweiler DP, et al (1998): Subtypes of reading disability: Variability around a phonological core. J Educ Psychol 90:347-373.
Moses P, Roe K, Buxton R, Wong E, Frank L, Stiles J (2002): Functional MRI of global and local processing in children. Neuroimage 16:415-424.
Paulesu E, Demonet JF, Fazio F, McCrory E, Chanoine V, Brunswick N, et al (2001): Dyslexia-cultural diversity and biological unity. Science 291:2165-2167.
Paulesu E, Frith U, Snowling M, Gallagher A, Morton J, Frackowiak RS, Frith CD (1996): Is developmental dyslexia a disconnection syndrome? Evidence from PETscanning. Brain 119:143-157.
Price C, Moore C, Frackowiak RSJ (1996): The effect of varying stimulus rate and duration on brain activity during reading. Neuroimage 3:40-52.
Report of the National Reading Panel (2000): Teaching Children to Read:An Evidence BasedAssessment ofthe Scientific Research Literature on Reading and itsImplications for Reading Instruction VolNIHPub. No 00 -4754. U.S. Department of Health and Human Services, Public Health Service, National Institutes of Health, National Institute of Child Health and Human Development: Bethesda, Maryland.
Richards TL, Corina D, Serafini S, Steury K, Echelard DR, Dager SR, et al (2000): Effects of a phonologically driven treatment for dyslexia on lactate levels measured by proton MRI spectroscopic imaging. Am J Neuroradiol 21:916-922.
Rumsey JM,AndreasonP,ZametkinAJ,AquinoT, KingAC, HamburgerSD,et al (1992): Failure to activate the left temporoparietal cortex in dyslexia. Arch Neurol49:527-534.
Rumsey JM, Nace K, Donohue B, Wise D, Maisog JM, Andreason P (1997): A positron emission tomographic study of impaired word recognition and phonological processing in dyslexic men.Arch Neurol 54:562-573.
Salmelin R, Service E, Kiesila P, Uutela K, Salonen O (1996): Impaired visual word processing in dyslexia revealed with magnetoencephalography. AnnNeurol40:157-162.
Scarborough H (1998): Early identification of children at risk for reading disabilities. In: Shapiro B, Accardo P, Capute A, editors. Specific Reading Disability. Timonium, Maryland: York Press, 75-119.
Seki A, Koeda T, Sugihara S, Kamba M, Hirata Y, Ogawa T, Takeshita K (2001): A functional magnetic resonance imaging study during sentence reading in Japanese dyslexic children. Brain Dev 23:312-316.
Shaywitz BA, Shaywitz SE, Pugh KR, Mencl WE, Fulbright RK, Skudlarski P, et al (2002): Disruption of posterior brain systems for reading in children with developmental dyslexia. Biol Psychiatry 52:101 -110.
Shaywitz S (1998): Current concepts: Dyslexia. N EnglJMed 338:307-312.
Shaywitz SE, Shaywitz BA, Pugh KR, Fulbright RK, Constable RT, Mencl WE, et al (1998): Functional disruption in the organization of the brain for reading in dyslexia. Proc Natl Acad Sci USA 95:2636-2641.
Simos P, Breier J, Fletcher J, Bergman E, Papanicolaou A (2000): Cerebral mechanisms involved in word reading in dyslexic children: A magnetic source imaging approach. Cereb Cortex 10:809-816.
Simos PG, Fletcher JM, Bergman E, Breier JI, Foorman BR, Castillo EM, et al (2002): Dyslexia-specific brain activation profile becomes normal follow-ing successful remedial training. Neurology 58:1203-1213.
Skudlarski P, Constable R, Gore JC (1999): ROC analysis of statistical methods used in functional MRI: Individual subjects. Neuroimage 9:311-329.
Snow C, Burns M, Griffin P (1998): Preventing Reading Difficulties in Young Children. Washington, DC: National Academy Press.
Talairach J, Tournoux P (1988): Coplanar Stereotaxic Atlas ofthe Human Brain. Three-Dimensional Proportional System: An Approach to Cerebral Imaging. New York: Thieme Medical.
Temple E, Deutsch GK, Poldrack RA, Miller SL, Tallal P, Merzenich MM, Gab-rieli JD (2003): Neural deficits in children with dyslexia ameliorated by behavioral remediation: Evidence from fMRI. Proc Natl Acad Sci USA 100:2860-2865.
Temple E, Poldrack RA, Protopapas A, Nagarajan S, Salz T, Tallal P, et al (2000): Disruption of the neural responseto rapid acoustic stimuli in dyslexia: Evidence from functional MRI. Proc Natl Acad Sci USA 97:13907-13912.
Torgesen J, Alexander A, Wagner R, Rashotte C, Voeller K, Con way T (2001): Intensive remedial instruction for children with severe reading disabili-ties: Immediate and long-term outcomes from two instructional ap-proaches. J Learning Disabilities 34:33-58.
Torgesen JK, Wagner RK, Rashotte CA, Rose E, Lindamood P, Conway T, Garvan C (1999): Preventing reading failure in young children with pho-
nological processing disabilities: Group and individual responses to instruction. JEducPsychol 91:579 -593. Wagner R, Torgesen J (1987): The natureof phonological processesand its causal role in the acquisition of reading skills. PsycholBull 101:192-212.
Wechsler D (1974): Wechsler IntelligenceScaleforChildren-Revised. New York: Psychological Corporation.
Wechsler D (1981): Wechsler Adult Intelligence Scale-Revised. Allen, Texas:DLM Teaching Resource.
Wiederholt J, Bryant B (1992): Gray Oral Reading Tests. 3rd ed. Austin, Texas:PRO-ED. Woodcock RW (1987): Woodcock Reading Mastery Tests-Revised. Circle Pines,MN: American Guidance Service.
Woodcock RW, Johnson MB (1989): Woodcock-Johnson Psycho-Educational Battery-Revised (WJ-R). Allen, Texas: Developmental Learning Materials.
www.elsevier.com/locate/biopsychsevier.com/locate/biopsych